Power cuts are annoying. In an ICU, they're fatal
by Prajakta Ayade
It started with a news clip. Power backup at a Delhi hospital failed at the two-second mark. The oxygen support system went down. A newborn died. That's not a statistic. That's a child who never got a chance because somewhere in the chain between diesel barrel and generator, something slipped.
In the IT industry, when the server goes down, it's only economic loss. In a hospital, it can be a life loss. A crashed server costs money. A crashed generator in an ICU costs something you can't get back.
Here's what the fuel management process actually looks like at most Indian hospitals, and it's messy in a very ordinary, unglamorous way.
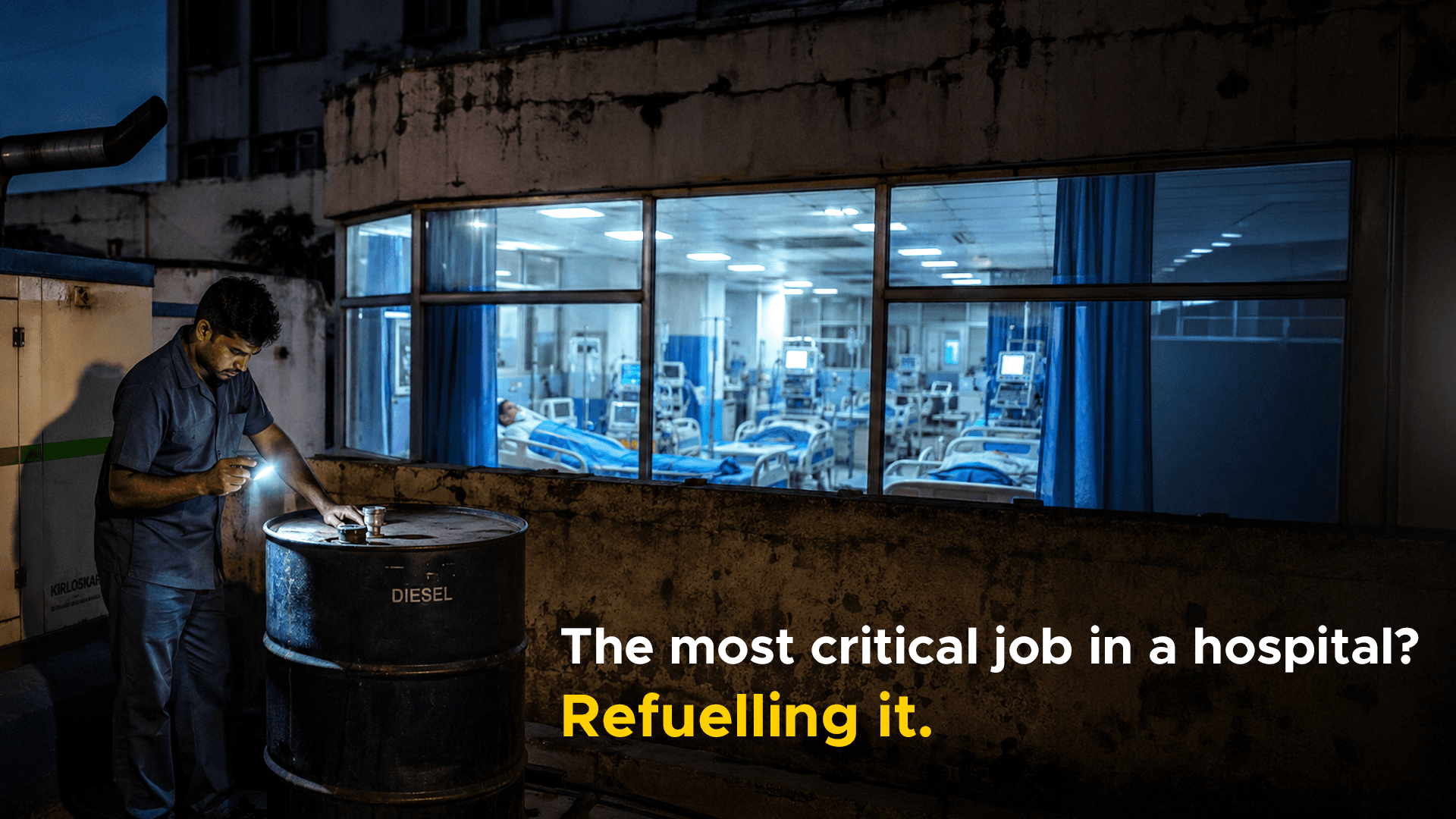
You grab empty barrels, load them onto a lorry, and drive to the petrol pump, often over an hour away. Add another hour if there's traffic. Get the barrels filled. Drive back. Offload. Then use a pump to manually transfer the diesel into the DG set tank.And while all of that is happening? You pray no power cut occurs before you're back, and that whoever's watching the pump doesn't miss a drop.
This isn't a broken system. It's no system at all. It's a hospital running critical life support on vibes and manual labour.
The people working in hospital maintenance rarely get a byline in these stories. But the anxiety they carry is real. One hospital worker put it plainly: there was always fear about whether enough diesel would be available, or whether the fuel level would suddenly drop without warning.
That background dread - day after day, shift after shift - is what it looks like when infrastructure fails at the systemic level. The generator doesn't fail in the dramatic movie-moment way. It fails slowly, through procurement delays, poor tracking, and a fuel barrel that ran low at the wrong time.
Repos in partnership with Cummins targets this whole problem smartly. The DG set itself tells you how much it's consumed. No more mental or physical parchi mathematics. No more 2am "is the diesel low?" panic. The data knows. The data orders.
One hospital confirmed it directly: after they started getting all the data, the fear was completely gone. That's not a small thing.
The bigger hospitals are sufficient enough to have a logistics team. But India has tens of thousands of small nursing homes and tier-3 district hospitals running on even thinner margins. For them, fuel management isn't inefficient, it's often just one person with a phone and a prayer.
The challenge of scaling automated fuel solutions to these institutions is largely economic, but the need is just as urgent, if not more so.
Automation doesn't just fix a logistics problem, it changes the psychological experience of people responsible for keeping patients alive. Progress is real here. But the work isn't done.
A power cut is inconvenient. In a hospital, it's something else entirely. It’s anxiety, worry, and life threatening.

